Many thanks to the talented Chris Snider for having me on the Just Talking Podcast this week. We discussed everything from the #doc to mental health to #MedX to how we chose our respective website names. Take a listen here!
diabetic online community

Whole Milk With The Disclaimers
This will not be my most popular blog post ever.
You may not agree with me. That is okay. In fact, it is a good thing. If we all nodded our heads along to the beat of the same drum in this world, well, we would be a boring orchestra. Renza wrote a great piece on this notion recently, which can be found here.
One of the largest issues we face in the United States today is the “battle of the egos.” We see it play out on our Facebook newsfeeds each morning:
“I’m voting for so-and-so and I must be right because it’s my opinion and I said so and I can scream louder than you!!!”
Yes, we have a right to say such things. But do we really need to completely write off the other side of the opinion in the process? If we do, quite frankly, we are only hurting ourselves. Very rarely in life are issues so cut and dry, 100% right or wrong. When politics falls into the gray zone, which it so often does, our greatest hope for the best world possible is to hear and consider all opinions, to put aside our personal biases and to think about what truly matters. We are way too quick to judge.
“He looked like a thug. He must have done something wrong. He would have shot first.”
We do not always pause to think of the psychosocial reasons why he is in the wrong place at the wrong time, or why we are in the right place at the right time- safe from injury or premature death, judging from afar.
Or, we roll our eyes dismissively, choosing to believe a social media rant from someone who has never seen combat, or public service in a rough neighborhood:
“The cop had more than a split-second to make a life-or-death decision; his life, or the alleged suspect’s?! He doesn’t go home at night sick to his stomach about taking another’s life, whether or not the the law supports his defense…”
We do not always concede that maybe, just maybe, in this particular case, we are speaking of a human being who perhaps acted in fear, rather than hatred.
At one point or another, we are all guilty of not placing ourselves in the other’s shoes. It is easier for us to say that one side is 110% wrong, and we are 110% right. If only morals and ethics were so mathematically easy…
We do not always think about how unique individuals are, how we cannot check them off like bubbles on the SAT, fitting a prescribed correct answer to each situation. Maybe there is none. Let’s sit in the scariness of that idea, together. Let’s be more loving and considerate than we have been as a society in recent weeks.
Admittedly, I have been disappointed in the diabetes advocacy world for similar reasons of us not seeing all sides of the equation lately. There are days where the #doc rallies and we do something that is so obviously good: honoring Kycie Terry this month, for example.
Regularly, we laugh together, cry together, share our lives with diabetes together. This is what makes us tick, what gives a distinct purpose to this disease in which we are, despite it all, somehow able to rise above.
My concerns, though, echo Tom Goffe’s wonderful post regarding the impending FDA decision on potentially dosing insulin based on Dexcom continuous glucose monitors (CGMs).
***(Disclaimer: I am not a medical professional; do NOT consider any of this blog post to be medical advice intended for treatment purposes.)
My personal opinion on diabetes management is more of a Libertarian view, if we want to talk politics. I am perfectly okay with individual patient-centricity in disease management. Diabetes falls on a spectrum of manifestations; what works for me, may not work for you, and vice versa. If you want to dose according to Dexcom and you are comfortable doing so, by all means, that is your prerogative, and I truly wish you all the success in the world.
Although I no longer use an insulin pump due to a freaky product defect hullabaloo that I encountered, I am happy for all of those who still have access and great results from insulin pump technology. That same mindset goes for those who experience phenomenal Dexcom CGM accuracy and ease of dosing insulin accordingly.
Every great innovation in society has come by those who are brave enough to take risks. Think no further than the Open APS and #wearenotwaiting folks in our own community. Their courage, creativity, and selflessness are beyond measure.
My #DoseWithCGM worry, though, begins with this being a rushed decision. CGM technology is not quite there yet in my opinion, and to have a trusted federal agency say that it is- under pressure from one side of the equation, rather than all sides- is a slippery slope.
Dexcom is- again, in my own opinion- the most innovative diabetes company in the market right now; I am absolutely confident that their technology will only go up from here; but we should not compromise safety and swap out access to other products in the interim. Generally-speaking, the government can curtail efficiency in health tech, but this is one rare occasion where it serves as a proper check and balance. As far as CGM dosing, don’t ask, don’t tell; do whatever you want (as an informed, experienced, safety-focused patient), but leave the government out of it.
There are the obvious physical dangers to insulin dosing, at any time and using any product as a baseline judge of BG; diabetes can be a conniving JerkFace.
Sure, I have 25 years of T1D under my belt and have a good sense of the disparities between my CGM’s interstitial fluid reading, and the blood sugar reading of my meter. But what about a newly-diagnosed family? What if Mom boluses 7-year-old Jenny based off of the CGM’s 300, when she is really 180? What if she is advised that this is an appropriate treatment approach by a federal agency set in place to keep her safe?
Sadly, insulin can be as life-taking as it can be life-preserving, and the reality is that it can sway from either extreme quickly and easily- through no fault of the patient’s or caregiver’s. This disease has a mind of its own, and even technology can never truly replace a fully-functioning pancreas. Again, #weneedacure. A real cure.
“I guess if you ate low carb and had a steady line at 100 all day, dosing off of CGM wouldn’t be that bad considering the tiny boluses,” I said, shrugging my shoulders.
“Actually, I think that could be more dangerous. There’s less of a BG cushion if something goes wrong,” a doctor replied.
Very true. That, or what about the T1Ds (myself very much included), who are not always smooth sailing at 100 mg/dL all day. Sometimes you wake up with a 55, rebound up to 224 when your liver releases sugar as the juice kicks in, correct and go back down to 78, eat lunch and sit at 162 for awhile, and then somehow see a 340 by dinner because your menstrual cycle begins and unleashes hormonal hell on your body. How in the heck can we ever expect a machine to keep up with that?!!
While I have seen the argument about meter reliability, I find it a weak one. Let’s attack the issue at the root cause: meters need to improve. But, they are still a better, more immediate guide than interstitial fluid ever will be. Together, the two are a wonderful pair, showing us real-time data, trends, alarms, and so on. I am not knocking either option, but I want to ensure that I have proper access to both in the long-term.
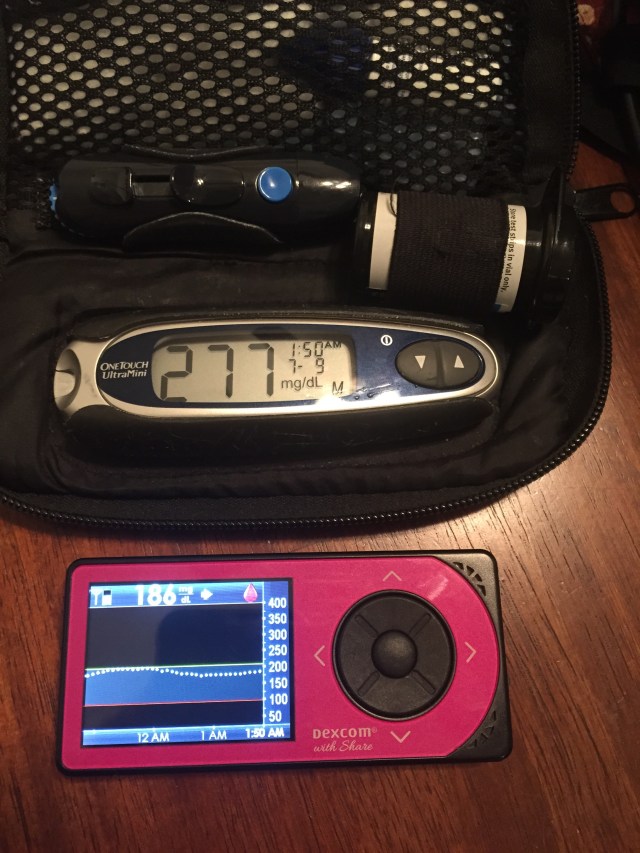
When I was normal person sick (NPS) last week, my CGM could not keep up. Neither could I, but I used all of the tools in my toolbox, to include my own diabetes intuition, to get out of the murky waters. Thankfully, I manually checked my blood sugar before dosing insulin at bedtime:
I in no way want to stifle innovation by expressing this opinion. I admire (and consider as friends) many of the advocates who are fully in support of this CGM dosing proposal. I also respect the major diabetes organizations which are onboard. Despite not agreeing wholeheartedly with their rationale in this case, I have no doubts that they want to see a better world for all diabetics. We all do, in our own ways.
My experience in healthcare leads me to believe that this decision will ultimately restrict our access to test strips, as insurance agencies will look to cut costs. And heck, as business leaders, they should; the ACA rewards and encourages cost reduction, and many consumers supported these measures vocally and at the polls. Regardless, this is beyond anxiety-provoking for so many of us. Test strips are ludicrously expensive already, and to imagine that we may be limited to a few checks a day to calibrate an imperfect CGM apparatus is maddening and disheartening, to say the least. Pass the coffee.
Imagine the current healthcare loop-de-loop. Imagine the Medtronic/UHC debacle. Actually, do not imagine- because we are already living it. And we know how unpleasant it is. Now pretend that your insurance has restricted your test strip supply, and you do not feel comfortable dosing via CGM. You have to get a letter from your endocrinologist, or perhaps a mental health care provider, indicating that you need more test strips to manage your chronic, lifelong condition which will never go away until there is a real cure. Nonetheless, you have to jump through this paperwork hoop every 3 months, missing time from work to argue with suppliers about why you need life-sustaining medical supplies. And maybe insurance will grant you 7 test strips per day instead of 2 when all is said and done… While this example is (hopefully) extreme, it is still possible. And it’s scary as heck for many of us.
“But Medicare won’t cover CGM. Or how will this affect the Libre?”
Again, I think we are attacking the wrong sources- deflecting one issue onto many others. By potentially limiting a test-strip-saavy demographic in the name of providing wider access to all is a total cop out. Instead, hold our government more accountable. CGM is a reliable tool, illustrated to be life-saving and absolutely quality of life-improving. For these reasons, Medicare folks (or swap in folks who want Libre access), deserve to have better technology on hand. But to substitute one option for another is silly, given that both CGMs and blood sugar meters have plenty of room for improvement in the current market.
Online polls and petitions do not represent the whole. From a science and data standpoint, they illustrate a sample demographic from which we can make some educated-inferences:
1.) Most of these people have computer/smart phone/internet access.
2.) This enlightens us as to their ballpark socioeconomic status.
3.) That gives us some idea of their access to and quality of healthcare.
Convenience samples are fine as long as biases are disclosed. We must say upfront that this is one side of the very large diabetes equation, and that this sample is not representative of The Whole. While we cannot all leave our fulltime jobs or school courses to lobby in front of Congress or the FDA, those representing us should be enlightened as to how we all feel, and should act accordingly.
As Erin Gilmer has respectfully pointed out on numerous occasions, there are marginalized demographics who cannot obtain the most basic of diabetes care: dental visits, for example. Yet we are up in arms over insulin pump collusion. Or, in this case, CGM dosing. The marginalized folks are not likely to be invested in this discussion because they do not have access to what is at stake; heck, they do not have access to the bare minimum. While we raise our voices, we must take caution not to further drown theirs out.
In many of the presentations of the CGM dosing issue on social media, I saw big fish in the diabetes pond introducing the topic as, “Here, this is good, hop aboard and get involved!”. This mindset is positive, for sure. But we are not whole if one of us is not heard, if different viewpoints are not given adequate opportunity to be discussed.
What about the school nurse who wrote into the debate on a Facebook status post? Did we listen when she said she would be uncomfortable dosing a child in her care at school based off of a CGM reading? Do we care?
On the flip side, if someone has great CGM accuracy and wants to lessen the finger pricks his type 1 toddler endures, am I hearing him out?
Que será, será. Whatever will be, will be. Ultimately, a decision will be made regarding the FDA and dosing with CGM. But we should all have a voice in it.
This is a long post and I surely will go to bed and realize I left out a few other big points. But this is food for thought for now. Although I am a little fish in the diabetes pond, it is my moral responsibility to use whatever platform I do have to improve life for diabetics. In my personal judgment, voicing this opinion has merit towards that cause.
I also promise to be upfront about my own diabetes biases. In the past, I have gotten on my soapbox and pledged up and down the river that we need a cure. But perhaps I have not listened to the other advocate on the soapbox next to me, who may be more focused on an artificial pancreas and who may feel that it is too painful to believe in a cure after years of disappointment. I have to respect that voice, too, because that person is part of The Whole.
So, here are my disclaimers:
1.) I can only represent my own opinions, but I hope that I can connect with others and help them by writing authentically and openly- whether we agree or disagree on various points.
2.) I will always hold out hope for a diabetes cure. Even if it does not benefit me in time, I want future generations to live in a better world. My blog focuses on this concept often, but please know that I respect everyone who strives for a better world for people with diabetes, however that world may be achieved.
3.) I will do my part to be more inclusive of The Whole. Firstly, I will feature more about cystic fibrosis-related diabetes (CFRD) on my blog. The CF community has so much to offer, and they have a valid seat at our diabetes table given CFRD/the risk of CFRD. Let’s learn more together. More to follow.
Too much skim or 2% milk leaves out a talented, diverse sample of people with diabetes. For the time-being, instead of taking my coffee very light (with cream), no sugar, I pledge to focus more on The Whole.
Thank you

Greater Love Has No One Than This
Greater love has no one than this: to lay down one’s life for one’s friends. John 15:13
Every day that we wake up as free individuals is because a Veteran/Service Member sacrificed for that freedom. Some make the ultimate sacrifice. Please pray for and reflect on them during Memorial Day, and every day.
Favorites and Forgiving Diabetes

My favorite post is one that mostly flew under the radar: 24. P.S. I forgive you.
This post describes how I chose to forgive diabetes for the bad and to reflect on the good I have received during my 24th “diaversary.” While it was not my most popular post of all time, it openly represents my emotions on a day that is always bittersweet.
Stephen’s short yet powerful comment on this blog post meant a lot to me, as did another I received via Facebook from the mother of a diabetic child who thanked me for writing the things that her son could not yet articulate at a young age. Those little moments make blogging so worth it. We can use our words to connect with and encourage others who face similar obstacles each day. #DOC in a nutshell!
Diabetes Campfire Stories
“Back in my day, we used pork-sourced insulin when I was diagnosed!” I may one day proclaim to my future grandchildren.
At this point in time, there will be a cure for diabetes and they will laugh off my fireside tales of the struggles of the past, oblivious to the hardships that generations before them have faced. Honestly, that’s how it should be if we aim to improve the world during our brief time here.
So many changes have occurred in diabetes treatments since my diagnosis just before my third birthday in the early 1990s. And I have not endured half of what rockstars like Supreme Court Justice Sonia Sotomayor have lived through regarding diabetes management processes! Change does not have to be a comparison battle, rather it should grant a clear perspective of just how blessed we are today despite a conniving autoimmune condition.
Almost one year ago I began using the Dexcom CGM (continuous glucose monitor) in the hopes of alleviating anxiety surrounding my diabetes. From the first day, I was absolutely floored by this product. Sure, it is technology and it is not the same as a properly-functioning pancreas. I have to carefully prep my insertion sites to avoid blistering rashes. And I am still waiting on my winning lottery ticket so that I can make my first purchase: a fulltime nurse who will check my blood sugar at night and will perform Dexcom insertions on me so that I do not have to do the one-handed pretzel move to get a sensor in my lower back.
Despite these minor issues, Dexcom is, in my humble opinion, the best quality product on the diabetes market. Due to many diabetes hurdles this year, I cannot boast of an A1C that drastically improved while on Dexcom, but I can say that my mental anguish regarding diabetes has lessened substantially thanks to Dexcom’s accurate readings. That, my friends, is half the battle. I still fear overnight lows, but I am much more confident that I will wake up thanks to Dexcom rattling and alarming from an empty coffee mug on my nightstand. I owe my life to Dexcom, as do many others. In the past, we all had to make do with what we had, and plenty of us survived prior to CGMs. But Dexcom is an added safeguard that makes life less complicated. It is the sort of change that is easy to embrace.
The Dexcom Facebook group was my true introduction to the diabetic online community. For the most part, this group is wonderfully supportive and non-judgmental- a place where we can all feel at home. We are able to share our scary moments and our triumphs with an audience who “gets it.” As I ventured off into the blogosphere, I fostered genuine friendships with others in the community, but I will always have Dexcom to thank for being the springboard to finding some of my largest supporters in fighting diabetes.
In grade school my mother used to drive to the auditorium to check my blood sugar every day at lunch. These were the infamous NPH and R days, and lunchtime was primetime for lows. My mother recalls seeing me file into the cafeteria with the rest of my class looking white as a ghost; she does not know how I had enough energy to even walk on some occasions when my blood sugar hovered in the 30s and 40s. There was no Dexcom back then to alert my teacher to the rapid decline.
On the playground in fourth grade, Michelle spoke the unfiltered truth. “I’m sorry that I didn’t invite you to my sleepover for my birthday. You could come if you weren’t diabetic, but my Mom doesn’t know how to take care of your diabetes so you can’t sleep over.”
In fairness to Michelle’s Mom, after twenty-four years of diabetes, I’m still trying to crack its code. I give her credit for recognizing that this disease is much more serious than an herbal cure remedy. Perhaps she could have coached her child on her delivery of the bad news a little more, but we can’t always have it all.
When I see the parents of children using Dexcom CGM post in the Facebook group about little Joey or Susie attending the first big sleepover of the school year, it never fails to bring tears to my eyes. Those kids put up with enough pokes and prods, fingersticks and pump site rotations, Dexcom insertions and limited cake consumption that they warrant having some fun with their friends every once in a while. They deserve to stay up all night eating popcorn and watching movies, forgetting that diabetes exists while Mom and Dad rest comfortably at home watching the steady line of the Nightscout Project’s Pebble watch display or the Dexcom Share apps.
Enjoy that good type of change. Remember the freedom that this product affords us, even on the days where the calibrations seem a bit off. After all, we are dealing with type one diabetes; diabetes’ “calibrations” to everyday life are rarely on the mark. Innovative products like Dexcom CGM allow us to live life in the moment, to have an additional security blanket onboard, to do things that diabetics in the past may not have been able to do.
To the parents of the kids going to the sleepovers where Dexcom gets the invite, too: Your kids will thank you for allowing them to just be kids one day when they are old enough to realize the sacrifices that you made for them. One day we will all sit with our respective families around the campfire and talk about that first sleepover as a diabetic, the first time fast-acting insulin was introduced, and so on, until we can finally talk about the first big meal after the cure.
Keep up the good work.

“Shots, Shots, Shots, Shots! Everyyyybodyyy!!”
(Thank me later for getting that LMFAO classic stuck in your head.)
May 6 will mark six months since my return to multiple daily injections (MDI), or, as I like to say, “shots.” Let’s call it like it is, people. It’s sticking a needle in your arm, butt, back, stomach, leg many times per day to deliver life-sustaining medication. It is not a cure, but it gives us life each day.
At a recent doctor’s appointment I proclaimed, “This rollercoaster isn’t working. I need to return to the pump!”
To which my doctor countered, “And you told me the same thing about the pump before you went back on shots, Ally!”
I responded with a stunned face that only a googley-eyed emoticon can convey. My doctor was right. Diabetes is not as simple as insulin pump versus shots versus Afrezza versus whatever floats your boat.
If I have learned anything in the past six months, it is just how different everyone’s diabetes is and just how different our treatment methods may be- whether out of personal choice or simply out of necessity. I’ll give another plug for Spare a Rose here: Most of us in the #doc are blessed to have any access to insulin, never mind the added bonus of having some flexibility in treatment options.
With that said, I know I seem like a broken record about the insulin pump. I want to set things straight here once and for all, while providing an update about my shots journey for those who may be interested.
Insulin pumps, when functioning optimally, are amazing devices. Going on the pump in high school opened up a whole new world to me. My parents breathed a sigh of relief that I could enjoy being a dorky kid with a bit more freedom back then. There are things that I miss immensely about insulin pumping: fine-tuning insulin doses, temporary basals, basal adjustments in one minute flat, carb-count/correction factor/insulin on board “wizards,” stability in blood sugar values on the good days.
If the pump works for you without many issues, all the more power to you. I want you to use whatever makes you feel healthy and happy- the same goals that I want for myself. In my rare case, going on shots had to serve that immediate interest in order to save my health. Do what works for you.
You can achieve a healthy lifestyle on shots, but it is more of a clunky, awkward sort of dance. Once that Lantus is injected, it’s there for the day. On Friday, my pancreas decided to rev up a notch (sarcasm), and for some odd reason I could not get my blood sugar to rise all day despite having taken the same dose of Lantus that I take every single day and hardly bolusing Humalog. I force-fed myself almost all of the leftover Easter candy to no avail. Good Lord did I miss the temp basal feature of the pump then! I longed for the personalized touches of modern technology that brick and mortar insulin injections simply do not afford.
I would ultimately like to ease into an “untethered” regimen of background Lantus in case of pump failures coupled with insulin pump usage again. However, this is quite complex, and we are not quite there with the shots yet. More details need to be worked out in terms of my basal and bolus plans. We are not settled into our comfort zone at this time, but we will get there. For now, we are enjoying the fact that insulin is getting into my body without technological glitches causing ketones each day, a freedom that I will never take for granted again.
Many topnotch brainiac doctors have looked into my pump issues. We know that the product did not work for me personally. But we also know that a pump-centric solution has not yet been provided. Right now, we do not need to add another factor to the equation. We’ll give shots a shot (see what I did there?) for another few months, at least.
I find myself daydreaming about a cure so often now: the party on the tropical island with the entire #doc; the sugary drinks consumed without having to stop and bolus- whether that be via insulin pump or shots; the happy kind of tears.
As a child when that elusive diabetes cure was “ten years away” (cue inside diabetic joke laughter), my father used to tell us about the enormous cure party we would have. There would be a table in the middle of the front yard with a sledgehammer on it. We would smash my blood glucose meter, syringes, and other diabetes supplies into tiny pieces to signify victory over a vindictive disease.
The sentiment was well-intentioned, although today I must admit that I laugh a bit at that particular daydream. If I were cured tomorrow, all of those diabetes supplies would immediately be donated to people who needed them in the interim. The supplies have nobler uses than being crushed by a sledgehammer.
We should be thankful for the supplies that we have keeping us alive right now. If an insulin pump does its job for you, perfect. If Afrezza is your drug of choice, inhale away. If shots suit you better, go for it. However you choose to do so, just fight the good fight until there is a cure.
Please keep those cure daydreams alive by continuing to advocate so well. #weneedacure
Try.
Try.
Dictionary.com says
“to attempt to do or accomplish”
“to put to a severe test”
“subject to strain, as of endurance, patience, affliction”
“to attempt to open (a door, window, etc.) in order to find out whether it is locked: Try all the doors before leaving.”
Fear.
Dictionary.com says
“the feeling or condition of being afraid.”
I fear spiders.
I fear insulin- too much and too little and not finding that happy medium dose.
I fear carbohydrates- too many or too few.
My biggest fear, though, is misconception.
If something “bad” ever happens diabetes-wise, others might think that I didn’t try.
This is why,
despite the fears,
brush the spider off the car windshield.
Say a prayer and take the insulin.
Eat the carbohydrates.
Treat the lows and the highs.
Until there’s a cure, we must
“Try all the doors before leaving.”
Try.
Short and Sweet
If you have wanted to get more involved with the diabetic online community (#doc) but are not quite sure how to do so, today is a good day to dive right in. We don’t bite!
Use the hash tag #IWishPeopleKnewThatDiabetes (brought to us by Kelly @diabetesalish) to document what you want others to understand about diabetes. Advocacy starts with the first tweet, Facebook post, blog writing session, and so forth. And advocacy can happen anytime, not just today. We’d love to have you onboard!
Insulin Angels in Hotel Mini Fridges
Please note: I was asked as a member of the diabetic online community to provide feedback on Insulin Angel and I am happy to do so. I did not receive compensation in any form for writing this blog post.
Let’s be honest, no one designed hotel mini fridges with the intention of storing insulin at safe temperatures. I was always under the impression that the original hotel mini fridge engineer wanted just enough tilt when opening the door to rustle a few alcoholic beverages and drive up your bill.
When most people open a hotel mini fridge, their objective is to quench their thirst. My main concern, however, is just how cold the beverages in the fridge may be- because if the beverages are borderline frozen, well, so is my insulin. You’ve all heard enough of my griping about ketones to last you a lifetime, so I’ll spare you the story this time around.
Bottom line: We all know that we need insulin to survive. Insulin that is too hot or too cold compromises the efficacy of the medication, and, therefore, endangers our health. Forgetting that insulin in the fridge when going out for the day is not highly recommended, either.
Mike Hoskins of Diabetes Mine provided a detailed take on Insulin Angel, a product which will alert users to unsafe insulin temperatures and inadvertent moments of forgetting to carry insulin by utilizing that handy dandy thing called modern day technology.
While I have not personally used the Insulin Angel product yet, I feel comfortable stating why I think this concept has potential:
1. Insulin Angel’s marketing strategy catches my attention because they are reaching out directly to those who their product will help: the diabetic community. Through crowdfunding, diabetics will drive this idea. Insulin Angel understands their consumers because they understand life with diabetes.
2. Have I mentioned how I just want a nice cold iced tea from the hotel mini fridge without thinking twice about insulin temperature yet?!
3. Fun activities like going to the beach in the summer should stay carefree. Let Insulin Angel do the worrying about insulin temperatures for you; you can correct any potential insulin temperature problem early on, rather than suffer the consequences later.
4. This product offers possibilities in a world that is not always diabetes-friendly.
As an example, diabetes is often considered a medically-disabling condition of military service. Although we have heard of people with diabetes who are able to remain in service in some capacity, one big reason why the military and diabetes don’t jive well is because of the need for insulin refrigeration; this proves technically-burdensome on deployments.
While I in no way, shape, or form am implying that Insulin Angel’s product will be helpful to allow diabetics to join or stay in the military (nor do I want to start a debate here), the main takeaway in raising the example is this: Previous/current limits on diabetics- whether self-imposed or societally-imposed- may one day be lessened due to this product.
Insulin Angel has the potential to give us another useful tool in our diabetes toolkits. It eliminates one of the many “I wonder if I’m high because of ______?” factors in that we can cross “unreasonable insulin storage temperatures/forgetting my insulin at home” off that list.
Think of it what you will. In the meantime, I’m ordering my #SaveHotelMiniFridges bumper sticker.

Sticks and Stones and Words
Many thanks to Douglas @salguodmai for being a supportive member of the #doc during the initial stages of writing this. And have I mentioned that he runs more miles in one weekend than I probably have in my lifetime?! Inspirational! Also, here’s a big shout out to Scott @Scott_InTheD for his Quotes that stick blog post, the concept of which I am borrowing here (with a somber spin on it- you’ve been warned!) with his permission.
“Sticks and stones may break my bones, but words will never hurt me.” Maybe on Opposite Day?
Diabetes scares the people who love us on occasion. In moments of weakness or misunderstanding, they may say things that hurt us, often unintentionally. This blog post has been batting around in my head for a few weeks now, and my inner English major keeps reminding me to let it out.
Words from others are only words. They do not have to define us, but they may explain things like the subliminal pain masked by epic Twitter rants or the irrational self-blame that we impose on ourselves when the CGM graphs look like Mount Everest. It’s sometimes there in the background, that internal voice that says you’re not good enough. The truth is that you are doing your best despite a rather difficult job as a substitute pancreas. Choice of words perhaps clouds this idea.
To quote Jay-Z, “Allow me to reintroduce myself.” Or at least to explain where I’m coming from on the bad days.
*****
“You’re a straight-A student, but you still can’t get it through your head!”
You’re right. I should have bolused more and eaten fewer carbs. But guess what? I’m going to be diabetic for a long, long time, and there’s always tomorrow. I messed up at a disease where you can give 110% and still not see the results that you want to see. I could do without the lecture.
^ That’s what I should have said. In reality, I probably walked away, did my homework to maintain those A’s, and hid my tears. And for the record, I’m still a straight-A student in grad school, and I still can’t get it through my head. But I know now that trying counts for a whole lot.
“If you didn’t eat _____, your blood sugar wouldn’t be 400.”
Because everyone loves a blood sugar value of 400…
“It IS your fault!”
No, it’s really not. My diabetic relative was simply trying to maneuver through a social setting, forgot about this pain-in-the-ass illness for a few minutes, and didn’t bolus until after the meal. You try doing this job and see how you like it.
“If this was Survival of the Fittest, you’d be long-gone by now.”
At the time, I laughed with the rest of the group. We were naïve high schoolers and the joke was not as tasteless as it looks on paper now. But there is that element of survivor’s guilt that still lingers. What if I had been born in another place or another time? He’s right; I wouldn’t have survived. But am I not ‘fit’ to survive as one of the ‘fittest’ now?
The consolation is that it isn’t another time, nor another place. It is here and now. I’m here. You’re here. Right now. We have survived as type one diabetics. It’s not a question of Why? but a question of What are we going to do with this life? We’re all doing a decent job in my book.
“Tons of people use the insulin pump. You’re the only one who had the problem, so it must be you.”
Look, diabetes is a blame game in society. We all experience this to some degree. What hurts is when people you love, who you’ve explained this to a million times before, take the cop-out option here. It’s easy to shrug pump problems or whatever it may be off on the user, the person with diabetes. None of us should ever have to defend actions we take to preserve our health, however unconventional they may be.
What I really want to say to you is that we both love each other. I do not want to keep rehashing the difficult stuff. You should inherently respect the decisions that I make regarding my own health. I may never know exactly why my pump problems happened, but they did. And every doctor and nurse involved came to the same conclusion: the issue was not caused by me, but by the product. I don’t want to have to prove it to you over and over again. I have moved forward, and I would like you to move along with me.
“I’ve learned a lot from watching you handle your degenerative disease.”
Who said it’s degenerative? Not me.
Sure, there’s the term “complications” which none of us like to hear. But the good news with diabetes is that it doesn’t always have to be “degenerative.” We have a lot of tools in our toolboxes at this stage of the game. These tools enable us to potentially live better than those with diabetes in the past may have lived.
Diabetes will never be a walk in the park, for me at least, but I refuse to go down without a fight. And I also know that if it does become “degenerative,” it is not my fault. It will hurt, yes, but it is not my fault. There are too many outside factors that affect diabetes to hold myself solely accountable. For starters, I’m snitching on faulty islet cells, stress, hormones, inaccurate carb counts, exercise, not enough exercise, and many more variables which are all guilty as charged. But heck, there’s nothing “degenerative” about a heart and soul that refuses to stop fighting the good fight- whether we are speaking about diabetes or any other challenge. Keep doing your thing, #doc.
“If I were managing someone else’s diabetes and could take insulin freely with no personal repercussions [hypos and hypers] experienced, I’d be a good diabetic.” -Me
“Are you aware of your language?” –My doctor
What? I didn’t swear, did I?
“Good diabetic” and “bad diabetic” don’t exist. There is the diabetic, or the person with diabetes, or whatever you choose to call yourself. There is the human being, who is more than diabetes. But let’s lose the self-destructive adjectives. There is only the doing-the-best-I-can-diabetic.
“Camping. Soccer in Montreal. St. Patrick’s Day Parade. There are so many things that I still want to do with you.”
My former college roommate said this genuinely and nonchalantly. We were planning future trips with friends and daydreaming of warm summer weather. What resonated with me was how much I wanted these things, too, and how far away they had seemed a few short months ago when it felt like diabetes had the upper hand. There are so many things that I still want to do with my friend, and with others, too. Thankfully, I’m going to be around to do them now, whether diabetes likes it or not.
“You’re not saying you can’t do something. You’re asking for help. We all do it. It’s life.” -My boss
Wait, I’m not weak if I ask for help? (Sarcasm)
Also, you are a really cool boss. (Not sarcasm. That was a significant learning moment for me.)
*****
My doctor and I are working on this thing that we call The Wall. Sometimes I let her remove a brick from the wall with a tiny chisel. Other times I try to deflect attention away to something of lesser pain value. I email her when I take a big bolus, a number that would have frozen me in fear in the past. A few bricks tumble down. We cheer via email and smiley face emoticons. Slowly but surely, our masonry skills are improving.
The Wall impacts how I feel about and handle my diabetes management at times. It’s a learning curve, and there are days when I am not proud of my behavior or my attitude. There are disheartened tweets which I later feel guilty about. Curse words may be said to people who I care deeply for. Feeling sick is no excuse, but sometimes feeling sick negatively affects my emotional inhibitions.
I joined the #doc with the promise of being transparent, so I’m confessing my stumbling blocks here and giving my written word that I want to work on this. I hope to one day sledgehammer the stumbling blocks- rather, the bricks- into smithereens.
If this post rings all-too-familiar to you, I want you to know that you can be a straight-A student and still not get it. Please know that it is okay. You are smart, not dumb. You are a fighter, not a failure.
Maybe diabetes is not yet meant to be fully understood? Just show up every day and work on it. That’s all anyone should ever ask of you.
