*Knock at the door*
I answered, in my pajamas with my hair totally disheveled, no coffee consumed yet. At the door was Anna*, a kindhearted employee of the hotel who was delivering fuel in the form of diabetes-friendly scrambled eggs… and, yay!, lots of coffee.
“What brings you to Cambridge?” Anna asked, striking up a friendly conversation.
I explained that I was a diabetes advocate there for a Pharma innovation event bringing together bloggers, media, pharmaceutical and diabetes industry folks, and others to work toward a better future for all people with diabetes.
Anna’s mind was blown. The excitement on her face said it all.
She had recently been diagnosed with diabetes and was in the process of sorting out treatment with her doctors. Anna was reinvigorated by the idea that other people with diabetes, and those who care about them, got together to engage so passionately. She had felt alone this entire time. Now, a spark of possibility was visible.
That interaction, albeit brief, stayed with me during the Lilly Diabetes Innovation Summit, the event I had briefly discussed with Anna. Anna was a reminder of why we need more hope infused into diabetes management for all types of diabetes (and, human beings!). Even with all of the knowledge, resources, and tools available, diabetes is a heavy presence to carry by oneself. Wherever the future takes us with diabetes, it should lessen this load in order to improve quality of life (QoL) for everyone touched by this condition.
***
Before I dive deeper here, let’s take an Intermission to talk disclosures, and my own related stances, for the sake of transparency:
I was invited by Lilly to attend the Diabetes Innovation Summit (sponsored by Lilly) at the Cambridge Innovation Center on May 3-4, 2018. I accepted the invitation. Lilly covered my travel, hotel, and incurred expenses for this event.
I am under no obligation to write about this, but, as you can see here, I willingly chose to do so. Opinions expressed are my own.
Advocates do this on their own free time. It is an honor to get to advocate like this, but I want to make sure readers hear directly that this involves a lot of hard work, too.
The devices which we viewed at the Innovation Center were prototypes, and constituted proprietary information. Lilly answered what they could, and acknowledged that they could not share everything related to development at this time. We were unable to take photographs of the laboratory, nor device prototypes. Thanks for your understanding.
I will try my best to convey what I learned in this blog post, much of which is paraphrased from the various sources we met while in Cambridge. I also live-tweeted important snippets of the event when time permitted. Please see my tweets from May 3-4, 2018, for that information.
The only diabetes story I can tell best is my own. I will never proclaim to represent The Whole community of diabetes because that would be an absolute disservice to everyone else’s individual diabetes, and life, experiences. That said, I do try to put a face to what makes diabetes advocacy so important: the human beings behind everything that we do, who deserve improved quality of life with diabetes. It is for this very reason that I believe advocates should always be present at events like this. I am grateful to have the opportunity to advocate at this level, and I want to thank Lilly for hosting us. Thanks also to MSL Group for coordinating our travel and schedules so that things ran smoothly.
I grapple often with my own nerdy healthcare interest in the good provided by Pharma [life-saving and life-sustaining prescriptions being one example, and good employees who have personally been kind to me throughout my own life circumstances being another], and the legitimate, persistent, life-altering concerns of access and affordability that the diabetes online community (DOC) knows firsthand. I could have articulated these concerns more clearly in the past, and I am owning that here. This time around, I brought up access whenever I could, as did many other advocates in attendance. Our points were received well [I do not believe various points of view necessarily need to be mutually exclusive], and I hope the future becomes brighter through this honest engagement.
This blog is thorough in its length and detail in order to provide you with lots of information, as requested.
This concludes Intermission.
***
The Summit kicked off on Thursday morning with introductions at the Cambridge Innovation Center. In attendance were Lilly folks who worked on-site in Cambridge, as well as others visiting from the Lilly headquarters in Indianapolis. (There are currently about forty employees at the Cambridge Center as a point of reference). We also caught up with diabetes advocates and media writers- some old friends and others new fast friends for me.
As some background in layman’s terms, Lilly- together with external collaborators to be discussed later in this post- plans to create a “connected diabetes ecosystem.” Essentially and ideally, consumers can expect a “smarter” diabetes management system encompassed by a hybrid closed-loop insulin pump and/or an insulin pen with a computerized “brain” attached. Lilly stressed the urgency of a comprehensive design that allows users to simplify the amount of effort involved in daily diabetes management.
The bells and whistles supporting this ecosystem will likely include a distinct phone app software, algorithms relying on intelligent trend analyses, continuous glucose monitoring (CGM), blood glucose meter results, and, of course, the individual characteristics and experience of the user with diabetes, combined with their healthcare team’s wisdom. There was also heavy suggestion of a potential “coaching” program a la other diabetes apps like MySugr. For this description, I have paraphrased a bit from Wil Dubois of Diabetes Mine, who does a great job articulating the connected ecosystem details concisely here.
After breakfast and coffee, we took a tour of the laboratory. Lilly is the Willy Wonka of pharmaceuticals, whether in Cambridge or Indy, and I mean that respectfully. Every tool and gadget imaginable can be found in the Cambridge lab, and Lilly has the capabilities to make a fully-functioning product right there in one spot. This includes on the molecular level with insulin manipulation. Lilly can sketch a concept, generate a prototype, and produce a design all in a day’s work, with additives such as 3-D printing aiding this process. Growing up in the Boston area, I know firsthand how much brilliance and ingenuity is centered in the Cambridge hub, and Lilly has chosen to develop its systems here for good reason.
In the bioengineering lab, we spoke directly with the designers working on the Lilly products in the pipeline. We met a specialist in fluidics engineering, who was also the father of a child with type 1 diabetes. His job entails deciphering how fluids such as insulin will maneuver safely and effectively in diabetes technology, using various valves and pressures.
We moved on to the Formulation Lab and were instantly struck by that all-too-familiar perfume scent otherwise known as “Insulin.” Here, giant vats of insulin and biologics can be tweaked to ensure safety and efficacy under certain circumstances, such as temperature stability and absorption areas/rates which drive outcomes and value.

One photo that was okay’ed to take outside of the lab: A live VLNS lab rat, white coat and goggles on point! ^
Next up was the Lilly Panel Question and Answer Session, in which Lilly employees provided us with more detail about the ecosystem, and where it plans to take us. For as long as I can remember, various connections of mine affiliated with Joslin Diabetes Center in Boston have said, “You have *got* to meet Dr. Howard Wolpert!” Well, finally, here was my opportunity.

Dr. Wolpert is now working at the Lilly Cambridge Innovation Center, and he lived up to all of the good things others have said about him. I got to chat further with him at dinner, and was totally impressed with his empathy and understanding for what we go through day to day with diabetes. After all, he is married to a researcher with type 1 diabetes, so he gets it. At the Lilly panel, Dr. Wolpert acknowledged how diabetes management has not aligned well with patients’ lives and individual nuances in the past, and Lilly’s innovation is an opportunity to change that for the better.
We also heard from Lilly’s Matthew Clemente, Chief Technology Officer; Rhett Alden, Chief Digital Architect; Kevin Cammack, Senior Brand Director at Lilly Diabetes; and Marie Schiller, VP of Connected Care and Site Head in Cambridge.
Multiple daily injections (MDI) are a market access point for the connected ecosystem. Selling points of the smart insulin pen include dosing suggestions based on tracked meal, exercise, and stress (measured by cardio rates) insights. Bluetooth and phone app guidance help the user to have some of the perks formerly only available with insulin pumps, while maintaining the simplicity of using insulin shots. While the design is still in the works, the pen may be in the form of a disposable platform, or possibly a small attachment piece.
Rapid usability feedback sessions, in which Lilly designers garner input from consultants and patients, drive the user-centered design approach. Personalized preferences may be honored with on/off, opt-in/opt-out toggle features. For example, not everyone may want constant notifications or loud alarms, and users may be able to adjust these options accordingly. If their interests change the following week, they can update selections to reflect this.
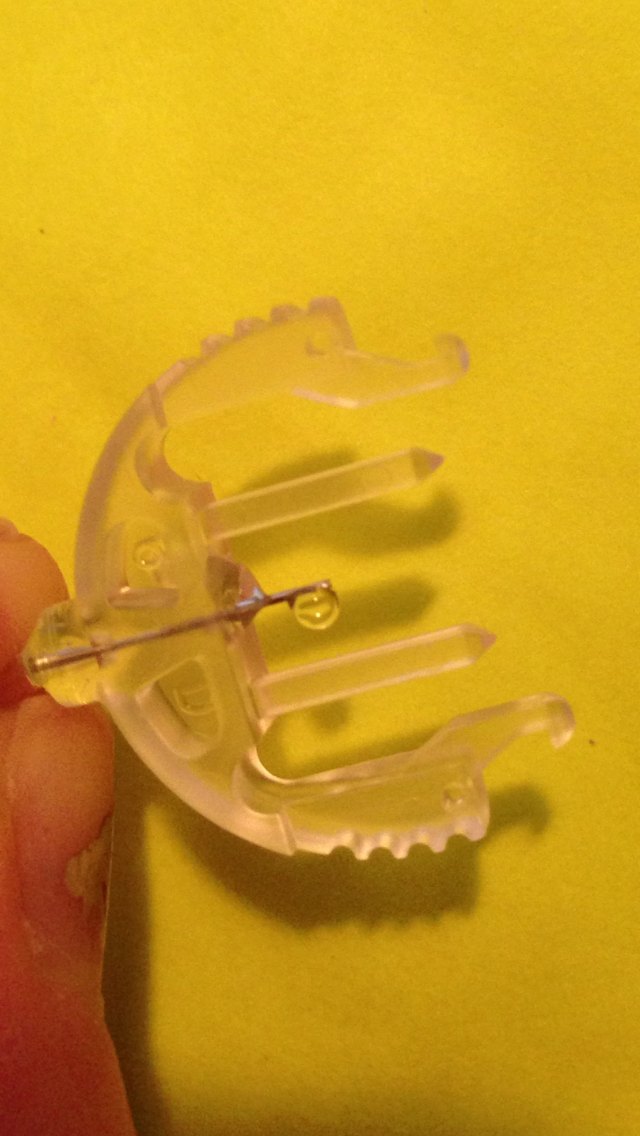
We were among the first people in the world to see Lilly’s automated insulin delivery prototype. In terms of length, width, and height, the pump prototype reminded me of the small Altoids tin shown in my palm in the photo below, if only the tin were circular. Flexibility, usability, safety, and “upgradability” were all important factors in Lilly’s design. Lilly aims to make diabetes management simpler, not just for “uber-users,” but for anyone of any health literacy background.
This pump can be worn in the usual injection/infusion site areas of the body. The pump’s short tubing will connect to standard Luer Lock infusion sets already in existence, but we are pushing hard for Lilly to design their own infusion sets as well. The option to secure the pump directly to the body with medical tape, similar to how many of us wear the Dexcom transmitter, is a possibility. I also hope to see a pump clip in the future.
While there will be smart phone interoperability with this pump, the pump can also run in automode if the controller is not present. (Currently, there is no screen included on the body of the prototype pump itself).** The efficacy of certain features is still being worked out, but one example in mind is a button on the pump’s outer shell** with pre-set bolusing capabilities. So, for example, if you lose your smart phone in a taxi after a wild bachelorette party, you might still be able to press a button and give yourself a pre-determined dose of insulin as needed.
On the flip side, safety could be an issue there. For example, you might have thought you pre-set the “button dose” to 0.25 units of insulin, but in reality, it had been set to 1 unit many months ago. Suddenly, the lost phone in the taxi cab is not such a big deal… There is also the idea that people are rarely detached from their phones nowadays, which bolsters the notion of phones homing the algorithms. I give Lilly tons of credit for being cognizant of these scenarios and actively working towards user-friendly, reliable, safe, innovative features. Lilly knows insulin well, but they are also proving to take the various elements of insulin’s delivery to new heights.
The pump will be piston-based with a flexible reservoir, and can hold 3 milliliters (mL) of insulin volume. Sites will be intended for three days of use. Dexcom G6 will communicate with this pump, and a model-predictive control algorithm will guide the way. Clinical studies are currently ongoing. How one will obtain Lilly’s hybrid closed loop system when the product arrives on the market is still in the works as well. A journalist in attendance noted the benefits of healthcare providers writing a prescription in one fell swoop, which would cover all of the moving pieces for the automated system.
Similarly to the way Anna’s breakfast delivery re-fueled my hungry stomach (and spirit), Lilly’s ecosystem is sort of like ordering room service for your rebellious pancreas. The keyword we heard the most while in Cambridge was FLEXIBILITY. Lilly recognizes that each person with diabetes is a unique individual, and management styles should reflect that accordingly. By catering to users’ personal preferences, Lilly hopes to make engagement easier. Diabetes management features, a la carte, so to speak. For the advocates in attendance, this is all awesome, so long as the ultimate price tag is more reasonable than hotel room service mark-ups.
As noted previously, Lilly’s pump will connect with standard Luer Lock infusion sets already in existence on the market. Having experienced the havoc-wreaking of defective insulin pump infusion sets repeatedly in the past, infusion set reliability is huge to me in any diabetes innovation going forward. The fanciest pump in the world is not worth much if insulin is not getting absorbed into the human body properly. Among others in attendance, I also encouraged Lilly to consider using their engineering brainpower to create their own high-quality infusion set product. I feel so adamantly about this that I have offered to meet with Lilly to discuss this further, as I am only a short car ride away from the Innovation Center. And I sincerely hope we make a point to follow up on this together.
All that said, when I was sick on the couch with ketones while going through the faulty infusion set fiasco (not developed by Lilly) a few years back, I never could have imagined I would get the chance to discuss the design of future products directly with the manufacturers. On a personal level, this brought me full circle as to what I have endured with diabetes technology, and how I can play my own small part in making things better because of these stories. Health tech is positively life-changing when it works as intended. But we have to do our best to ensure safety and quality so that human beings are not hurt in the process when bumps in the road appear. Lilly was absolutely cognizant of these concepts and open to hearing us out, and I believe this reinforces another reason why advocates are always needed at these events.
A Lilly panel Q&A would not have been complete without diabetes advocates raising the issues of access, and raise the issues we did. I was proud of our cohort for our expression of a life and death topic in our community. Insulin is the fuel running these technological developments, and, as an essential for people with diabetes, insulin is the starting point from which other access flows.
I reminded the panel that Lilly is in a unique position as a diabetes pharmaceutical giant now dipping into other aspects of diabetes management and innovation. They have the ability to set the tone regarding access to this innovation, and, due to the sheer number of people living with diabetes worldwide, their business will be viable no matter what. Making these services available to diverse groups of all backgrounds – particularly those vulnerable in socioeconomic and psychosocial facets – would be an admirable route with positive ripple effects throughout healthcare.
To Lilly’s credit, they listened and acknowledged our points. Marie Schiller sticks out to me for repeatedly noting that any innovation Lilly develops is moot if it cannot get to the people it purports to serve (paraphrased here). Through various testing and outreach opportunities, Lilly intends to make access more equitable.
Day 2 brought us to the external collaborator panel, where we heard from representatives of Dexcom, DEKA Research and Development Corporation, Rimidi, and Canada’s McGill University.

In summary, the panel relayed their great trust in Lilly’s ability to make an advantageous product for the diabetes community. Heck, that’s why they are joining forces with Lilly! Dexcom’s Dana Cambra discussed how the Dexcom G6 has changed everything for the better, boasting a new algorithm, membrane, and applicator. Lilly’s Marie Schiller discussed how insulin is a “really hard molecule” in terms of manipulation, and how DEKA’s expertise can provide a mechanical solution. Rimidi offers an intuitive EHR (electronic health record) platform which could suggest certain treatment options (such as Lilly’s future ecosystem) to patients identified as possible candidates. McGill’s Dr. Ahmad Haidar is the brain behind the algorithms used in Lilly’s designs. Dr. Haidar emphasized lessening the diabetes managerial burdens we currently face through this technology.
“Adherence” data on insulin remains somewhat scarce. [I still do not love ‘compliance’ or ‘adherence’ terminology, as, arguably, the issues lie within our broken healthcare system much more than they do with patients’ willingness to feel better]. We can download pumps and CGMs, but that still only gives us a tiny glimpse into reality. Through clinical studies, Lilly will be able to garner more useful, in-depth information, to include smart insulin pen dosing details. Lilly’s partnership with Tidepool could be one example of how Lilly learns more about people with diabetes through data analysis.
This panel was as good a place as any to chime in about access. I wondered aloud how much our diabetes data is saturated by the health-literate, privileged folks who just so happen to be the type to engage with diabetes tech. I also asked how anyone- whether an informed blogger, or an Average Joe Diabetes, might eventually take the first step to gain access to this multifaceted diabetes management system. The short answer is that such points of entry are still being ironed out as the system develops over time.
In my opinion- earned by hours spent fighting with insurance, just like every other person with diabetes- solutions to these kinks need to be highly prioritized in order to make the Lilly ecosystem quickly accessible, and successful, for all. The advocates in attendance suggested that Lilly work closely with diabetes clinics and healthcare providers in various locations, treating diverse demographics, in order to support awareness and feasibility of these future options.
We also briefly discussed the healthcare industry trend towards value-based care. With healthcare providers and patients, alike, being impacted by outcomes data, innovation such as Lilly’s will have to prove its worth, too. I voiced concern- which goes far beyond Lilly’s innovation and more so towards this value-based trend in general- that there will always be patients, particularly in complex autoimmune disease situations, whose outcomes will not align with the extraordinary effort they put into chronic disease management. I asked the rhetorical question of how we will support them so that they do not fall through the cracks. Lilly takes angles like these into consideration when targeting therapies to deliver on individuals’ needs, and the short answer here is that they anticipate that their innovation and collaboration will prove helpful.
We later participated in a lively ideation session led by Matchstick LLC, complete with colorful graphics drawn on the spot by ImageThink. Here, our hosts picked our brains regarding design. For our example, we created our ideal smart insulin pen, complete with the likes of insulin dosing memory and suggested/predictive dosing capabilities; sound, which could be formatted to suit the user, and also to ensure safety (clicks based on number of units could help prevent or alert to inadvertent overdose, for example); and phone app support. The pen would likely be in a disposable format, rather than having a “smart” attachment, and it would hold 300 milliliters (mL) of insulin- mitigating insurance coverage arguments being one reason we leaned this way.

Smart insulin pen design poster by ImageThink. ^ Insert all obvious Friday afternoon jokes from the crowd, too.
I departed from the Lilly Summit feeling more optimistic than I have felt about diabetes technology in a long time. After going through my past insulin pump trials and tribulations, I need something new and exciting to hang my hope hat on, and I feel that the Lilly innovation is that hope. We require more options in diabetes-land, and Lilly is a Goliath that can compete in a revolutionary manner.** I want everyone with diabetes to have access to optimal tools for diabetes management, and my hope also rests on the idea that we can make quality of life better for all of us through such accessible means.
Thanks again to Lilly for hosting us!
For more information on the Lilly Diabetes Innovation Summit, check out these previously-published pieces linked from:
diaTribe
Stacey Simms
Diabetes Mine
* Name changed for privacy purposes.
** Updated later on May 21, 2018, for clarity purposes.